We all know the importance of protein and carbs, but have you ever considered the importance of micronutrients? In our latest X-Change, written by Professor Graeme L. Close and his team, we will take a look at the importance of micronutrients for health, growth and athletic performance.
Read the full X-Change article here or download the pdf via the button below
Key Points
- Vitamins and minerals are essential for health, growth and athletic performance. They may be obtained from the diet or (in the case of Vitamin D) from sunlight.
- Micronutrients include vitamins which are classified into water-soluble (B and C vitamins) and fat-soluble (A, D, E and K vitamins).
- Athletes may face micronutrient deficiencies, with vitamin D, B12, folate, magnesium, iron and zinc being common concerns.
- Deficiencies in micronutrients can negatively affect athletic performance and health.
- Adequate dietary intake is essential and blood or urine testing may be needed to identify deficiencies.
- Athletes with high energy expenditure may need increased micronutrient intake, while others may require specific dietary strategies.
- The absorption of minerals can be affected by factors like phytates, oxalates and fibre in foods.
- Specific water-soluble and fat-soluble vitamins play distinct roles in athletes’ health and performance.
- A comprehensive assessment of athletes’ energy requirements, dietary habits and nutrient status is essential for addressing micronutrient deficiencies and optimising performance.
Introduction
Vitamins are organic compounds that support health, growth and reproduction. They are required to be consumed through the diet, in small amounts, to prevent clinical deficiencies and declines in health (Fogelholm, 2015). Most vitamins are required to be obtained from dietary intake, as the body is unable to synthesise them. Vitamins are broadly classified based on their solubility, with A, D, E and K termed fat-soluble and vitamins B and C termed water soluble vitamins.
Minerals are inorganic substances that support physiological functioning (Fogelholm, 2015). The daily physiological requirements of a mineral determines their classifications whereby daily requirements of ∼100 mg/day−1 are considered macro-minerals (these are NOT macronutrients), and include sodium, potassium, calcium, phosphorus and magnesium. On the other hand, minerals required at ∼20 mg/day−1 are known as trace elements and include iron, zinc, copper, chromium and selenium (Fogelholm, 2015). Figure 1 provides an overview of some of the key micronutrients and their functions.

A Brief History
Whilst the role of sports nutrition often focuses on macronutrients and subsequent total caloric intake, micronutrients can often be overlooked, despite being essential for health, disease risk and daily physiological processes. This is not a new consideration, though. In 1906, Frederick Hopkins recorded that animals could not live on protein, fat and carbohydrate alone (Hopkins, 1906). He highlighted that scurvy, rickets and other medical conditions were a consequence of ‘nutritive errors’ and, whilst not identified at the time, correctly attributed our dependence on ‘unsuspected dietetic factors’.
The use of trace elements such as iron, iodine and zinc for health was relatively common in the 19th century (Semba, 2012). In 1912, Casimir Funk was able to demonstrate that feeding pigeons a diet based on polished rice resulted in polyneuritis which could be overcome by simply supplementing the birds’ diet with rice bran which included the outer husk than is removed when polishing rice.
Funk hypothesised that the polyneuritis resulted from a lack of a vital factor (which we now know was thiamine or vitamin B1) which was found in rice bran. Funk also believed that some human diseases such as beriberi, scurvy and pellagra could also be caused by deficiencies of vital chemicals found in food (Funk, 1912). At the time of this discovery, all of these vital factors had a nitrogen-containing component known as an amine and, as such, he termed these food borne factors vital amines which was eventually termed vitamins. Later research demonstrated that not all vital amines did contain an amine group and as such the final ‘e’ was dropped from vitamines and the name became “vitamins”.
The history of micronutrients can in fact be dated back much further than 1912. Indeed, some ship captains in the 15th century proposed that some fruits prevented scurvy, although it was not until 1930 that ascorbic acid was isolated and identified by Albert Szent Gyogyi (Carpenter, 2012).
By this time, over 2 million sailors had reportedly died between the 16th and 18th century alone (Carpenter, 2012) demonstrating the critical role that micronutrients play in the diet. Since 1912, there has been an abundance of literature concerning micronutrients. Despite the disease risk, there remains a lack of experimental research conducted in elite athletes, and so our understanding of requirements of micronutrients on this specific population is limited. Indeed, a recent review on micronutrients for athletic performance (Beck et al., 2021) discussed only five micronutrients (iron, calcium, vitamin C, vitamin D and vitamin E), likely due to the sparsity of literature within athletic populations.
Terminology explained
The first noted daily recommendations for micronutrients were made in 1941 when the Food and Nutrition Board published the Recommended Dietary Allowances (RDAs) (National Research Council, 1989). The RDA is today defined as “the levels of intake of essential nutrients that, on the basis of scientific knowledge, are judged by the Food and Nutrition Board to be adequate to meet the known nutrient needs of practically all healthy persons.”.
In the UK, Dietary Reference Values (DRVs) have been set since 1992. These include:
ESTIMATED AVERAGE REQUIREMENTS (EARS)
The EAR is an estimate of the average requirement of energy or a nutrient needed by a group of people (i.e. approximately 50% of people will require less, and 50% will require more).
REFERENCE NUTRIENT INTAKE (RNIS)
The RNI is the amount of a nutrient that is enough to ensure that the needs of nearly all the group (97.5%) are being met.
LOWER REFERENCE NUTRIENT INTAKES (LRNIS)
The LRNI is the amount of a nutrient that is enough for only a small number of people in a group who have low requirements (2.5%) i.e. the majority need more.
SAFE INTAKE
Safe intake is used where there is insufficient evidence to set an EAR, RNI or LRNI. The safe intake is the amount judged to be enough for almost everyone, but below a level that could have undesirable effects.
Figure 2 provides an illustration of the key terminology with regards to micronutrients and health requirements in humans.
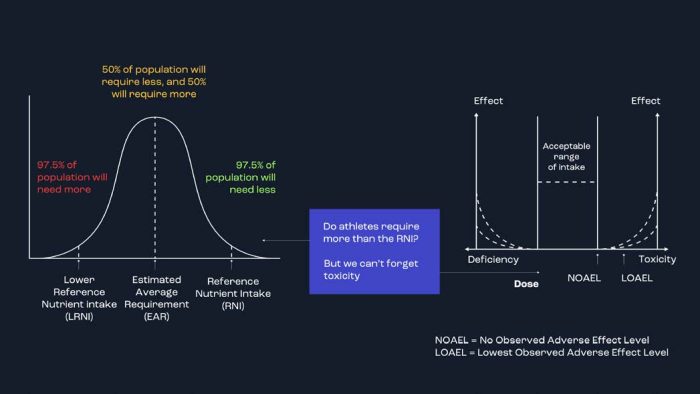
Figure 2. Sufficient, optimal, or more? What are we aiming for or trying to avoid with athletes? Athletes should initially look to ensure they have no micronutrient deficiencies before looking to increase intake above and beyond typical values. More is not always better and particularly high doses of certain micronutrients can lead to toxicity issues.
HOW MUCH DO WE NEED?
Typically, the goal of a well-balanced diet in a healthy individual is to obtain all of the micronutrients in recommended doses for normal bodily functions and avoid deficiencies. There is limited data examining deficiencies in athletic populations and the prevalence is likely to vary between clubs, countries and continents. Although there is no data to suggest that widespread micronutrient deficiencies exist in athletic populations, particular deficiencies have been more commonly seen for vitamin D, B12, folate, magnesium, iron and zinc (Jordan et al., 2020). athletic performance. Athletes are more likely to be deficient in a particular micronutrient if they also have a low daily energy intake or restrict certain food groups from their diet. It may not always be practical, or relevant, to assess vitamin and mineral concentrations from blood or urine samples, and so initial approaches from practitioners are likely to focus on dietary intake recording and analysis.
If an increase in energy expenditure does require an increase in micronutrient intake, this can likely be met in most cases by a general increase in total energy intake. Vitamin C intake, for example, correlates with energy intakes up to >4500 kcal/ day (Figure 3). However, there are also some micronutrients that may be more difficult to attain through typically dietary means. Worldwide, iron deficiency is one of the most common dietary deficiencies (Clark, 2008) and, for athletes, it has been shown that low-to-moderate calorie diets often fail to be sufficient for athletes to meet the RNI (Figure 3).
There is, though, a need to update and expand the relationships between typical dietary intakes of athletes and the risk of deficiencies across the range of micronutrients.
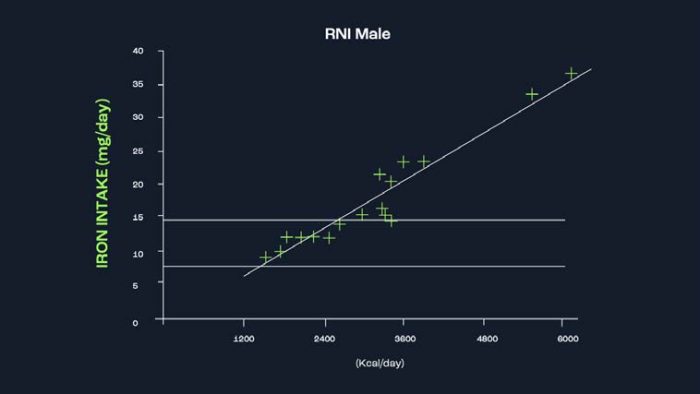
Figure 3. The relationship between total calorie consumption and micronutrient intake(redrawn from Erp-Baart et al (1989). For many micronutrients, the RNI can be met when athletes consume adequate daily calories (assuming there are no major food group omissions). However, in some instances, such as iron, deficiencies are much more likely with even moderate calorie intake.
However, is it optimal for athletes to only avoid deficiencies? Is ‘more’ better in some circumstances? Equally, will typical intake values help athletes avoid deficiencies? It is well understood that increases in energy expenditure due to exercise training requires increases at the macronutrient level, so do athletes therefore require greater amounts of micronutrients?
A number of minerals are also lost via sweat during exercise (Consolazio et al., 1963). Does this require athletes to increase their dietary intake? Whilst there are a limited number of studies investigating the effects of increased intake of certain vitamins and minerals on athletic performance, there is in some cases a lack of data.
Absorption
The absorption rates of different minerals can vary. It is difficult to know the absorption rates for individuals and specific micronutrients as they depend on certain factors such phytates, oxalates and fibre in foods which can inhibit mineral absorption (Deal & VanReken, 2017). Here are some examples of typical absorption rates for certain minerals:
IRON
Typical absorption rate:
Approximately 10%
Factors that can affect iron absorption:
Consuming iron-rich foods with vitamin C-rich foods (e.g., citrus fruits, bell peppers) can enhance iron absorption (Skolmowska et al., 2022). Avoiding consumption of iron inhibitors (e.g., tea, coffee, calcium-rich foods) during meals can also improve iron absorption (Hallberg & Hulthén, 2000).
CALCIUM
Typical absorption rate:
Approximately 30%
Factors that can affect calcium absorption:
Consuming calcium-rich foods with vitamin D can enhance calcium absorption. Adequate stomach acid production is also important for calcium absorption, so maintaining a healthy digestive system is beneficial (Booth & Camacho, 2013). Many non-dairy foods contain high quantities of calcium but have a lower fractional absorption. For example, several foods of plant origin contain anti-nutritional factors, such as oxalates and phytates that adversely affect the absorption of calcium and other minerals (Popova and Mihaylova, 2019). Some studies have shown that as little as 10% of calcium contained within spinach is (Shkembi and Huppertz, 2021).
ZINC
Typical absorption rate:
Approximately 20-40%
Factors that can affect zinc absorption:
Consuming animal-based sources of zinc (e.g., meat, seafood) generally have higher bioavailability compared to plant-based sources. Soaking, fermenting, or sprouting plant-based foods can improve zinc bioavailability (Sandstead, 1994). Alternatively, phytate, a natural substance found in plants, can severely decrease intestinal absorption of zinc and is considered the main nutritional inhibitor of zinc. However, phytate can be broken by phytase increasing the bioavailability of zinc. In contrast to sheep and pigs, that possess the ability to break down phytate with endogenous intestinal phytase, humans possess very low amounts of the enzyme and thus rely on phytase from plants and microorganisms. Furthermore, phytase found in plants, particularly in grains, can be activated during food processing and fermentation making zinc more bioavailable (Maares and Haase, 2020, Lönnerdal, 2000).
MAGNESIUM
Typical absorption rate:
Approximately 30-40%
Factors that can affect magnesium absorption:
Adequate stomach acid production is important for magnesium absorption. Consuming magnesium-rich foods (e.g., nuts, seeds, whole grains, leafy green vegetables) can enhance absorption (Rude & Shils, 2013). Plant sources can affect the absorption of magnesium. This occurs since they contain non-fermentable fibres like lignin and cellulose, along with oxalate and phytate. Seed germination, soaking of legumes and grains, and the implementation of sourdough methods in bakery processes initiate the enzymatic
action of endogenous phytase. This enzymatic action results in in a reduction of phytate (Schuchardt and Hahn, 2017).
MEASUREMENT AND MONITORING
There is currently no single gold standard method for assessing micronutrient intake and biological availability for individual athletes. Additionally, individual factors such as age, sex and medical history should be considered when interpreting the results. There is also a lack of data regarding micro and macro cycle changes in these markers for athletic populations. In addition, serum / plasma carries newly absorbed nutrients and those being transported to the tissues and therefore typically reflects recent dietary intake. Therefore, serum / plasma nutrient levels usually provides an acute, rather than long term, biomarker of nutrient exposure and/or status. The magnitude of the effect of recent dietary intake on serum / plasma nutrient concentrations is dependent on the nutrient, and where necessary, can be reduced by collecting fasting blood samples (Gibson, 2021). A potential framework for a more holistic assessment has been suggested and includes: anthropometrics and body composition assessment; biochemical analysis of targeted biomarkers (typically from blood samples) in the clinical assessment to include investigation of relevant symptoms suggestive of possible deficiencies; dietary analysis of nutrient intake; environment scans including socioeconomic status; living arrangements, grocery shopping and cooking abilities; transportation, training regimen, education, culture, psycho-social support system, religious practices and personal belief systems.
PRACTICAL TIP
In our experience working with athletes, there are 5 major risk factors that contribute to micronutrient deficiencies in athletes that practitioners should look out for
- Eliminating food groups from diets either due to food dislikes, allergies or ethical reasons.
- Low calorie diets often utilised when attempting to reduce body fat (i.e. boxers, jockeys).
- Very low-fat diets, which could affect the fat-soluble vitamins
- Lack of variety in the diet.
- Lack of sunlight exposure (including constant use of sunscreens or protective clothing).
It is important to identify if your athlete falls into any of these risk factors and if so particular attention must be given to their micronutrient intake and strategies developed to reduce the risk of deficiencies.
VITAMINS AND MINERALS FOR ATHLETES
Although it is beyond the scope of this review to give an in-depth overview of each major dietary micronutrient, we next highlight some of the research for each as is relevant to athletes.
Water-soluble vitamins
VITAMIN C
Vitamin C has been of considerable interest to athletes due to its potential role in immune support and as an antioxidant. A large body of evidence now exists showing that regular daily supplementation of vitamin C has no effect on reducing the number of coughs and colds individuals experience, but could reduce the duration and severity of these illnesses if vitamin C is supplemented at the first show of symptoms (Hemilä & Chalker, 2013).
With regards to its effectiveness as an antioxidant, vitamin C supplementation of 200–1000 mg/day has been shown to reduce oxidative stress in exercising participants (Mason et al., 2020). This may be beneficial during periods of intense exercise, when oxidative stress is likely higher and could have damaging effects. However, complete suppression of oxidative stress may not be the optimal approach in all circumstances.
It is now known that oxidative stress plays a role in the molecular signalling responsible for some adaptations to training. Complete suppression of this oxidation can therefore blunt our responses to training (Figure 4). In one review, vitamin C supplementation at doses of 1000 mg or more per day significantly impaired sport performance in 4 out of the 12 studies included (Braakhuis, 2012). Given that there is little evidence to suggest that vitamin C can improve exercise performance, it likely means that athletes should target the RNI through dietary means, and only consider higher dose supplementation if symptoms of coughs and colds are experienced.
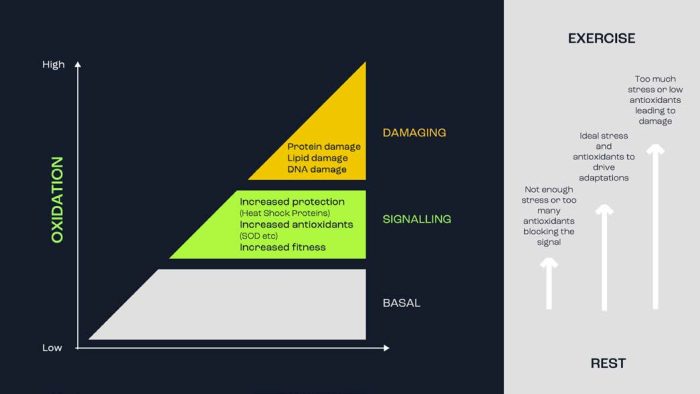
Figure 4. It has been shown that oxidative processes are involved in both molecular signalling and adaptation to exercise training, as well as potential cellular damage. While there are many factors, the ‘dose’ and exposure is likely a key differentiator between the two.
VITAMIN B1 (THIAMIN)
Thiamin is a water-soluble vitamin that, amongst other functions, plays a role in carbohydrate metabolism. Early studies showed that restriction of dietary thiamin (alone or in addition to restriction of other B vitamins) led to reductions in exercise performance (Van der Beek et al., 1988), possibly due to its role in carbohydrate metabolism. However, it has been recently shown that muscle thiamin content did not influence muscle glycogen metabolism during exercise (Sato et al., 2020). It had also been previously shown that a short-term, high dose of thiamin did not improve muscular performance (Doyle, Webster, & Erdmann, 1997) nor endurance performance (Webster, 1998). Data examining adequacy of dietary intake of athletes is limited and mixed. From a group of Dutch athletes that do not take daily supplements, ~38% were seen to not consume the suggested intake (Wardenaar et al., 2017). A study of Brazilian para-athletes showed that the prevalence of inadequacy was 5-6% (Sasaki & da Costa, 2021). It is important for athletes and individuals engaged in regular exercise to ensure adequate thiamine intake.
VITAMIN B2 (RIBOFLAVIN)
Riboflavin functions in the mitochondrial electron transport chain, predominantly in the metabolism of fatty acids. Earlier data suggested that riboflavin status may decline during a short period of increased physical activity (Soares et al., 1993) and there is some data indicating that dieting alone or exercise alone may increase riboflavin requirements above the RDA. It also showed that dieting plus exercise increases the requirement even more (Manore, 2000). However, it has been shown that athletes can maintain good for riboflavin when adequate energy is consumed (Woolf & Manore, 2006) and it appears that dietary inadequacy is not particularly common. In athletic groups, one study found ~13-16% were seen to
not consume the suggested intake (Wardenaar et al., 2017), which is similar to the 8-13% shown in another (Sasaki & da Costa, 2021).
VITAMIN B9 (FOLATE)
Folic acid is a vital vitamin that plays a crucial role in DNA synthesis and amino acid metabolism, acting as a cofactor for several enzymes. Folate is required during the process of cell division and so is important for growth, the synthesis of new cells, such as red blood cells, and for the repair of damaged cells and tissues (Molina-López et al., 2013). It may then be speculated that folate requirements might be higher with exercise, since damaged muscle tissue needs to be repaired. This should be of particular concern given that folate has regularly been shown in athletes to be one of the micronutrients most commonly consumed at levels below guideline recommendations (Volpe, 2007). For example, the prevalence of moderate folic acid deficiency assessed via serum concentrations (folate <5.9 ng/ml) was shown to be around 20% in elite Ethiopian runners, although there was no athlete with severe folate deficiency (<3 ng/ml). Lower total daily energy intakes and low intakes of fruits, vegetables and grains are suggested to be risk factors to low folate intake and deficiency.
VITAMIN B12 (COBALAMIN)
Vitamin B12, or cobalamin, is a vitamin produced by bacteria. It is responsible for red blood cell formation in bone marrow, maintenance of the immune system, enhanced neural signal transmission and increased synthesis of neurotransmitters and creatine (Krzywański et al., 2020). Whilst different thresholds for the classification of vitamin B12 deficiencies have been used, serum samples collected from over 200 elite athletes showed no athletes as being deficient (<200 pg/mL) (Krzywański et al., 2020). This same study suggested that serum concentrations between 400-700 pg/mL were optimal for haematological measures, and vegetarian and vegan athletes. Figure 5 illustrates how some of the water-soluble vitamins may be ingested via foods.

Figure 5. Water soluble vitamins, dietary sources, and the reference nutrient intake
Fat-soluble vitamins
VITAMIN A
Vitamin A was among the first vitamins to be discovered and is widely recognised as an important factor in the maintenance of healthy cells and tissues (Semba, 2012). There is limited evidence to suggest that vitamin A deficiency is more common than other micronutrients. The average vitamin A intake was below the RNI in a group of academy football players (Naughton et al., 2017) and inadequacy was seen in up to 48% of Dutch athletes (Wardenaar et al., 2017). Athletes may caution against high-dose supplementation, though, as high doses of vitamin A may be associated with reduced bone density (Tanumihardjo, 2013). There are very few studies investigating the effects of vitamin A deficiency on athletic performance. An early study showed no effect on running performance in men after 6 months of a vitamin A deficient diet (Wald et al., 1942).
VITAMIN D
As our understanding of vitamin D has increased, so has the interest in it and its use as a supplement. Vitamin D has a multitude of roles and benefits to athletes, least of which include bone health, muscle function and immune support. For a full breakdown of vitamin D, check out The Nutrition X-Change Vol 1 with Dr Daniel Owens and Prof Graeme Close.
VITAMIN E
Like vitamin C, vitamin E has gained interest for its antioxidant properties. However, like vitamin C, most research has shown no consistent benefits of chronic supplementation on exercise performance (Beck et al., 2021). There is also limited evidence to suggest that there is any significant prevalence of dietary inadequacy of vitamin E in athletes (Jordan, Albracht-Schulte, & Robert-McComb, 2020). Figure 6 illustrates how some of the fat-soluble vitamins may be ingested via foods.

Figure 6. Fat soluble vitamins, dietary sources, and the reference nutrient intake minerals
CALCIUM
Calcium is important for muscle and cardiovascular function. Calcium is also lost through sweat during exercise (Martin et al., 2007). It may then be considered that athletes would benefit from calcium supplementation. It has been shown that supplementation can attenuate post-exercise reductions in blood concentrations of calcium, but there is no strong evidence to show any direct effects on exercise performance (Martin et al., 2007).
Calcium has also been identified as one of the important nutritional factors for bone remodelling and optimal bone mineral density during growth and maturation, and throughout adulthood (Gordon et al., 2017). Inadequate calcium intake has been suggested to be more common from the dietary minerals that have been assessed (Volpe, 2007). Deficiencies have been suggested to be caused by entire food groups high in calcium (Fig 7) being reduced or avoided (Naughton et al., 2017).
MAGNESIUM
Magnesium is an essential mineral and is a cofactor for hundreds of enzymatic reactions involved in processes such as cellular energy production and storage, protein synthesis, and cell growth and reproduction.
Data on athletes’ typical intakes has shown mixed results with both adequate and inadequate amounts being suggested depending on sport, gender and caloric intake (Newhouse & Finstad, 2000).
One potential issue faced by individuals is that magnesium absorption is only between 30-50% (Rude, 2000). This may explain why it has been shown in a group of bodybuilders that their serum magnesium concentrations were below reference values, despite dietary intake above recommended values (Kleiner, Bazzarre & Ainsworth, 1994).
IRON
Considering the importance of iron contributing to red blood cell generation, cellular energy production and immune system support, it is perhaps surprising how the prevalence of iron deficiency has been seen to be up to 30% in female athletes (Sim et al, 2019). But, when you consider the typical dietary intake levels (Fig 7), you can see one of the reasons why such deficiencies occur. For a full breakdown and overview on iron status testing, dietary intake and supplement strategies, see The Nutrition X-Change Vol. 13 with Prof. Peter
Peeling.
ZINC
Zinc is involved in the biochemical processes supporting life, such as cellular respiration, DNA reproduction and maintenance of cell membrane integrity, and is required for the activity of more than 300 enzymes. The average dietary intake of zinc seems to meet the recommended levels, although, when examined individually, a significant number of athletes in various sports (ranging from 52.6% to 93.7%) are reported to have zinc intake below the recommended levels (Jordan et al., 2020). There is limited research on supplementing zinc-deficient athletes. It has been shown that supplementing athletes with 20 mg/day of zinc for 6 weeks did not result in any changes in health status or performance data, although specific details on performance data were not provided (Grosshauser et al., 2006). Figure 7 illustrates how some of the minerals may be ingested via foods.

Figure 7. Fat soluble vitamins, dietary sources, and the reference nutrient intake minerals.
Conclusions
Athletes are regularly exposed to intense training stress, which necessitates matching their energy intake with the energy demands. However, several factors contribute to inadequate replenishment of energy needs, leading to potential deficiencies in vital vitamins and minerals. This puts athletes at an increased risk of nutrient deficiencies. To address this risk, practitioners should utilise a comprehensive framework that assesses the athlete’s overall energy requirements, current dietary practices, and biological and clinical status.
This assessment helps identify the need for nutritional intervention when a nutrient deficiency is detected. If a deficiency is identified, it is crucial to consider the appropriate approach to resolve the issue. This includes considering factors such as nutrient recommended daily intake, supplement dosage and timing, concurrent consumption of other foods and potential interactions between food and drugs. These considerations are vital for optimising the effectiveness of the chosen approach to correct the nutrient deficiency.
A former professional Rugby League player, Graeme is now Professor of Human Physiology at Liverpool John Moores University. His research is focused on basic and applied sport nutrition, where he has published ~175 papers and review articles. Graeme’s current research areas are the effects of Vitamin D and cannabidiol (CBD) on skeletal muscle function, the effects of weight-making on health and performance, and the metabolic and nutritional demands of elite rugby. Graeme is accredited with BASES and SENr and is a fellow of both BASES and ECSS. Graeme is currently the High Performance consultant to England Rugby and the Head of Performance Nutrition for The DP World Tour Golf. He has previously held roles with Pakistan Cricket, Everton, Aston Villa, West Bromwich Albion and Nottingham Forest football clubs, The Lawn Tennis Association, British Ski and Snowboard, Heavyweight Boxing and many other elite sports people and organisations. Graeme regularly appears on television (BBC’s Trust Me I’m a Doctor, ITV’s The Truth About Food) and radio (BBC Radio 4, BBC Radio Merseyside) discussing nutrition for health and sports performance. Graeme is the Lead Nutritionist and Scientific advisor to Nutrition X and has played a key role in the design and development of the entire Nutrition X product range.
Dr. Jamie Pugh (PhD) is a post-doctoral researcher at Liverpool John Moores University. Through his research, he has investigated at the effect exercise can have on the gastrointestinal system and, in more recent work, looked at the effects probiotic supplementation can have on endurance athletes. He has also worked as a consultant nutritionist and physiologist for a number of professional teams, marathon runners and extreme endurance athletes.
Samanvita is a postgraduate researcher at Liverpool John Moores university investigating the pathophysiology of gastrointestinal barrier function in response to exercise and the potential protective effects of probiotic supplementation.
Fernando is a PhD student in Biomedicine from the University of Córdoba, Master in Physiology from the University of Barcelona and Master in Biomedicine from the University of Córdoba. Dietitian-Nutritionist for elite athletes. Currently, he is also a professor of Human Physiology, Nutrition and Metabolism and Sports Nutrition at several Spanish universities, both at undergraduate and graduate levels. He has written more than 50 articles and book chapters.
Andreas has worked at the highest level of elite professional sport since 2014 and is currently a performance nutritionist working within the Premier League. He has previously worked with a number of Championship Football Clubs with extensive experience of working within different performance teams and with international players. Alongside the roles within football, Andreas’ team sport expertise extends to rugby, where he has worked with both the national England Rugby Union (RFU) and League (RFL) sides with pathway and senior sides, respectively. Andreas completed his PhD at Liverpool John Moores University in the area of applied scientific research, where his thesis focussed on translation of research into practice.
References
Beck, K. L., von Hurst, P. R., O’Brien, W. J., & Badenhorst, C. E. (2021). Micronutrients and athletic performance: A review. Food and Chemical Toxicology, 158,112618
Braakhuis, A. J. (2012). Effect of vitamin C supplements on physical performance. Current sports medicine reports, 11(4), 180-184.
Carpenter, K. J. (2012). The discovery of vitamin C. Annals of nutrition and metabolism, 61(3), 259-264.
Clark, S.F. (2008). Iron deficiency anemia. Nutrition in Clinical Practice, 23, 128– 141.
Consolazio, C. F., Matoush, L. O., Nelson, R. A., Harding, R. S., & Canham, J. E. (1963). Excretion of sodium, potassium, magnesium and iron in human sweat and the relation of each to balance and requirements. The Journal of nutrition, 79(4), 407-415.
Deal, L.L., & VanReken, D.W. (2017). Clinical: Food-drug interactions. In L.K. Mahn & J.L. Raymond (Eds.), Krause’s food and the nutrition care process (13th ed., pp. 122–138). Saint Louis, MO: Elsevier.
Doyle, M. R., Webster, M. J., & Erdmann, L. D. (1997). Allithiamine ingestion does not enhance isokinetic parameters of muscle performance. International Journal of Sport Nutrition and Exercise Metabolism, 7(1), 39-47.
Funk, C. (1912). The etiology of the deficiency diseases. The Journal of State Medicine (1912-1937), 20(6), 341-368.
Gibson, R. S. (2021). Principles of nutritional assessment. Oxford university press, USA.
Gordon, C. M., Zemel, B. S., Wren, T. A., Leonard, M. B., Bachrach, L. K., Rauch, F., ... & Winer, K. K. (2017). The determinants of peak bone mass. The Journal of pediatrics, 180, 261-269.
Hemilä, H., & Chalker, E. (2013). Vitamin C for preventing and treating the common cold. Cochrane database of systematic reviews, (1).
Hopkins, F. G. (1906). The analyst and the medical man. Analyst, 31(369), 385b-404.
Jordan, S. L., Albracht-Schulte, K., & Robert-McComb, J. J. (2020). Micronutrient deficiency in athletes and inefficiency of supplementation: Is low energy availability a culprit?. PharmaNutrition, 14, 100229.
Kleiner, S. M., Bazzarre, T. L., & Ainsworth, B. E. (1994). Nutritional status of nationally ranked elite bodybuilders. International Journal of Sport Nutrition and Exercise Metabolism, 4(1), 54-69.
Krzywański, J., Mikulski, T., Pokrywka, A., Młyńczak, M., Krysztofiak H., Frączek, B., & Ziemba, A. (2020). Vitamin B12 status and optimal range for hemoglobin formation in elite athletes. Nutrients, 12(4), 1038.
Manore, M. M. (2000). Effect of physical activity on thiamine, riboflavin, and vitamin B-6 requirements. The American journal of clinical nutrition, 72(2), 598S-606S.
Martin, B. R., Davis, S., Campbell, W. W., & Weaver, C. M. (2007). Exercise and calcium supplementation: effects on calcium homeostasis in sportswomen. Medicine and Science in Sports & Exercise, 39(9), 1481-1486.
Mason, S. A., Trewin, A. J., Parker, L., & Wadley, G. D. (2020). Antioxidant supplements and endurance exercise: Current evidence and mechanistic insights. Redox biology, 35, 101471.
Molina-López, J., Molina, J. M., Chirosa, L. J., Florea, D. I., Sáez, L., & Planells, E. (2013). Effect of folic acid supplementation on homocysteine concentration and association with training in handball players. Journal of the International Society of Sports Nutrition, 10.
Naughton, R. J., Drust, B., O’Boyle, A., Abayomi, J., Mahon, E., Morton, J. P., & Davies, I. G. (2017). Free-sugar, total-sugar, fibre, and micronutrient intake within elite youth British soccer players: A nutritional transition from schoolboy to fulltime soccer player. Applied Physiology, Nutrition, and Metabolism, 42(5), 517-522.
“Recommended dietary allowances.” (1989) National Research Council-National Academy Press: Washington, DC, USA .
Rude, R. K., Magnesium. In: Stipanuk, M. H., Ed. Biochemical and Physiological Aspects of Human Nutrition. Philadelphia: W.B. Saunders Company, 2000, 671– 685.
Sasaki, C. A., & da Costa, T. H. (2021). Micronutrient deficiency in the diets of para-athletes participating in a sports scholarship program. Nutrition, 81, 110992.
Sato, A., Sato, S., Omori, G., & Koshinaka, K. (2022). Effects of Thiamin Restriction on Exercise-Associated Glycogen Metabolism and AMPK Activation Level in Skeletal Muscle. Nutrients, 14(3), 710.
Semba, R. D. (2012). The historical evolution of thought regarding multiple micronutrient nutrition. The Journal of nutrition, 142(1), 143S-156S.
SCHUCHARDT, J. P. & HAHN, A. 2017. Intestinal Absorption and Factors Influencing Bioavailability of Magnesium-An Update. Curr Nutr Food Sci, 13, 260-278..
SHKEMBI, B. & HUPPERTZ, T. 2021. Calcium Absorption from Food Products: Food Matrix Effects. Nutrients, 14.
SKOLMOWSKA, D., GŁĄBSKA, D., KOŁOTA, A. & GUZEK, D. 2022. Effectiveness of Dietary Interventions to Treat Iron-Deficiency Anemia in Women: A Systematic Review of Randomized Controlled Trials. Nutrients, 14, 2724.

Written by
Professor Graeme L. Close